Table of Contents
The months leading up to medical school graduation are exciting, but also the beginning of the next chapter: The Match. The residency match process doesn’t have to be stressful — this free guide is meant to help you feel more informed and in control.
I’m Dr. Amar Mandalia. I’ve been through The Match myself, served on admissions committees, and helped hundreds of students find success in residency applications, so let me lead you stress-free through this process with some expert tips thrown in.
Our Physician Advisors match 99% of US clients and 88% of IMG clients into residency.
What Is the Match?
Match Week happens every March, when you find out if you got into medical residency. The residency Match algorithm is how the National Resident Matching Program (NRMP) pairs applicants with programs, based on both applicants’ and programs’ rank order lists (ROLs).
Many factors influence Match success, including:
- Specialty choice
- USMLE scores
- Med school GPA
- Strong personal statement
- Extracurriculars
- Demonstrating ACGME core competencies
- Working towards a PA vs. MD vs. DO degree
The Nobel Prize-winning algorithm-driven Match process was invented in the 1950s to standardize the process in medical students’ fourth year and improve outcomes for both students and programs. It has undergone improvements over the years and is still considered successful.
Prior to the Match, programs would individually extend offers to med students as early as their second or third year. The former process became highly competitive and much less fair.
Check out this webinar on how to match into your dream residency.
Match Process
The Match process is fairly straightforward, but it’s good to know the ins and outs of how it works, so you can boost your chances of success while decreasing your stress levels.
- ROL: After completing interviews at residency programs, you must submit a rank order list (ROL) of your preferred programs to the NRMP’s R3 system. Meanwhile, residency programs submit an ROL of their preferred applicants.
- Algorithm’s first attempt to match: The Match algorithm first tries to match applicants to their first-choice residency program at the top of their rank order list (ROL). If the program has also ranked the applicant on their ROL, and if there are open spots in the program that haven’t already been filled by applicants ranked higher by the program, then a tentative match occurs.
- (A tentative match means that the applicant will attend the program unless they are later displaced by the algorithm to make space for another applicant ranked higher by the program.)
- Algorithm’s continued attempts to match: If the applicant’s first-choice program hasn’t ranked them on their ROL, or if all the program’s spots are already filled by higher-ranked applicants, then the algorithm will move on to the applicant’s second-choice program. This process continues until the algorithm finds a tentative match or the applicant’s program list is exhausted. Couples Match adds an extra wrinkle to this; read more on Couples Match below.
- SOAP: If the algorithm doesn’t match you to any program, you’ll find out on Monday of Match Week. You have Tuesday through Thursday to apply and interview through the Supplemental Offer and Acceptance Program (SOAP) process. Basically, unmatched applicants pursue unfilled residency spots. Read more on SOAP below.
Once all applicants have either been matched, have had their ROLs exhausted, or have failed to match through SOAP, the Match process is over.
To learn more about how to make the best use of this matching algorithm for your specific circumstance, check out this helpful video on using the Residency Explorer tool by the AAMC:
ERAS Application
To increase your chances of matching into your preferred residency, applicants should prepare their ERAS application well before the submission date in early September. To learn more in-depth about the ERAS application, read this free guide.
In the past, the AAMC allowed supplemental applications for certain specialties, including secondary application questions. ERAS Supplemental Applications were eliminated for the 2023/24 cycle. However, for some specialties, there are now Specialty Questions included on the primary ERAS application.
Below are the various sections of the ERAS application for residency, which you need to fill out to be eligible for the Match:
- Personal and Biographical Information: Here’s where you input or confirm basic demographic and identity information.
- Experiences: This section allows you to list extracurricular activities outside of your grades, similar to the Works & Activities section on AMCAS. You may list up to 10 experiences, three of which you can identify as “most meaningful.” There is also a newer, optional section called “Impactful Experiences.” Optimizing this section can help match you to programs because residencies are looking for well-rounded individuals.
- Personal Statement: A personal essay lets residency programs know more about you beyond your coursework. Start writing your ERAS personal statement as early as possible. Use AI only to suggest edits, never to write out the actual words for you. A personal statement can be all the difference for Match Week. Pro tip: Keep a note on your phone or computer about experiences from medical school you want to include in your personal statement.
- Publications: Here, you will enter information about each publication you’ve been cited in. This section can make or break your match with highly competitive residencies. You’ll select publication types from the AAMC’s predetermined list or select “None” if you have no appropriate entries to submit.
- Letters of Recommendation: 2-3 letters of recommendation (LORs) from mentors or professional supervisors satisfy most residency programs’ requirements for interview invites and matching. Don’t wait until right before the application process to request letters. For more info, the Association of American Medical Colleges has details about the format of the letter. This UCSF page has great information on what to include in the letter.
- Medical Student Performance Evaluation: Also called the MSPE or “Dean’s Letter,” this is where your medical college will submit a unique letter detailing your academic history, educational progress, personal strengths, and any negative actions taken against you. Each school has different policies on the MSPE process, so I recommend asking your Dean’s office about the MSPE. The school will notify the applicant and generate the letter for you to upload to ERAS.
- Medical School Transcript: The medical school transcript must be uploaded to ERAS directly from the applicant’s Designated Dean’s Office of their medical school.
- ECFMG Status Report: This report is for international medical graduates (IMGs) only. The Educational Commission for Foreign Medical Graduates (ECFMG) Status Report verifies the ECFMG Certification status. The report contains information like your USMLE/ECFMG identification number, exams passed for certification, and more important information about your ECFMG status and, therefore, your Match eligibility.
- Photograph: You have the option to include a photograph with your application. The photo should be 2.5 x 3.5 inches, with a 150 dpi resolution and a file size of 150KB — or in digital terms, 375 pixels x 525 pixels. I recommend including a professional headshot to slightly increase your chances of an interview invite. No selfies, please.
- USMLE and COMLEX-USA Transcripts: You may upload your USMLE and/or COMLEX transcripts with your application. While this is technically optional, many programs will not consider applicants who do not include these scores. Particularly as Step 1 is now pass/fail for USMLE test-takers, and 90% of residency programs “never” or “seldom” consider students for matching who fail Step 2 on their first attempt, your board exams are a major factor in your application.
Do I need to submit a CV? You don’t need to create a separate CV apart from your application. The CV compiled in the MyERAS portal is an auto-populated document formatted to include information found elsewhere on your application.
If you’d like to have a copy of this document, you can download it by selecting “View/Print CV” in the same area where you can print the entire ERAS application.
Read Next: Medical School vs. Residency: What to Expect
ERAS Timeline
Most residency positions are offered through the Electronic Residency Application Service (ERAS). The timeline varies each year, but it generally starts in June, culminates with The Match in March of the following year, and the ERAS cycle officially ends in May.
The 2025-2026 ERAS Residency Timeline is as follows:
| June 4, 2025 | ERAS 2026 season begins at 9 a.m. ET. You can now gain access to MyERAS. |
| Sept 3, 2025 | You should have fine-tuned your application well before this date and started your interview prep. Residency applicants may begin submitting MyERAS applications to programs at 9 a.m. ET. |
| Sept 24, 2025 | Residency programs are allowed to start reviewing MyERAS applications and MSPEs in the PDWS at 9 a.m. ET. |
| Mar 16, 2026 | Match Week begins, and students will be informed as to whether or not they matched to a residency program. |
| Mar 20, 2026 | The final day of Match Week, known as Match Day. |
| May 31, 2026 | ERAS 2024 season ends at 5 p.m. ET. |
Programs typically start reviewing applications at the end of September into early October. Interviews are conducted from October through February.
The Main Residency Match occurs over the process of one week in March, known as Match Week, peaking on Match Day — Friday, March 20, 2026.
Craft your ERAS personal statement with the help of a professional writer and a Physician Advisor with admissions committee experience. No limits on messaging, hours, or edits.
Match Program Outliers
While most programs operate through ERAS and The Match, I know of several programs that operate outside of this structure or alongside it:
- The Military Match: Applicants in the military must complete a rank order list (ROL) and submit an application to the Joint Service Graduate Medical Education Selection Board (JSGMESB), which is in charge of the match for military-run residencies. Military medical students may also apply for civilian residencies through ERAS, but are still required to submit an application and ROL to the JSGMESB, who ultimately decide whether they will be allowed to train in a civilian setting. The timeline for the Military Match is significantly shorter than for ERAS — the application deadline is usually October 15th, and results are released on December 15th.
- The Urology Match: Certain applicants interested in urology apply through ERAS, and rank lists are due in early January. Some programs use NRMP, and some use a urology match program. Match Day is towards the end of January or early February each year.
- Ophthalmology Match: Applicants looking to go into ophthalmology need to apply through the Central Application Service (CAS) and match through the SF Match in January or early February.
- Preventive Medicine: Certain applicants who want to work in preventive medicine must contact individual programs to determine their process. Some use ERAS, and some use a unique application service. Many use a separate matching service outside the NRMP called the Standardized Acceptance Process (SAP). The SAP deadline for rank lists is around January 23rd. Match Day is around February 5th.
ERAS vs. NRMP
It is important to understand that the residency application process and the residency matching process are administered by two separate entities:
- ERAS (Electronic Residency Application Service) is administered by AAMC (Association of American Medical Colleges)
- ROLs and The Match are administered by the NRMP (National Resident Matching Program)
You’ll need to register for both systems for most residency applications to match.
ERAS allows you to package your application and send it to programs, which in turn will offer you interviews.
NRMP allows you to make and submit a ranked program list from your most to least desirable residency training programs. Then, the algorithm matches you.
Related Read: Average Residency Salary by Specialty + Job Level
Residency Interview
Interviews for medical residency typically start in the late fall to early winter. I would aim to interview at as many programs as possible to increase your chances of matching somewhere.
Since COVID, many residencies now conduct their interviews virtually, removing a major financial barrier that was previously in place. However, some programs are returning to the in-person interview day.
You can expect to find these types of questions and prompts in a typical residency interview:
- Why did you want to become a physician?
- What makes you want to be a [specialty]?
- What are your greatest strengths and weaknesses?
- Describe a research project you were involved in.
- Name three things wrong with the U.S. healthcare system, and propose some fixes.
- What is your interest in this specific program?
- How do you manage stress?
- What other subspecialties did you consider?
- What is the most interesting case you have encountered?
- What would you do if you saw a senior resident or attending do something wrong?
- Please explain any gaps or discrepancies in your education.
- What three words would your patients describe you with?
- What three words would your colleagues describe you with?
- What’s your approach to educating your patients?
- How will you contribute to the diversity of our program?
Now, let me offer some free tips about your residency interview day:
- Attire: Dress professionally. Your clothes should be neat and presentable. They should not distract from you as a candidate. As far as jewelry, don’t wear anything that draws attention away from your message as an applicant.
- Stature: Sit upright and lean in, just like you would when speaking to a patient. Body language conveys interest, so leaning back with crossed arms will send the wrong message.
- Framing: If you’re participating in a virtual interview, ensure you’re in a brightly-lit area and that your background appears professional. Having interesting items in your room that are visible on camera can be an excellent conversation starter.
- Ask questions: Every interview will end with the same question: “What questions do you have for me?” The most common wrong answer is to walk away without asking your interviewer questions. Be prepared with some questions of your own, such as queries about their workplace culture or what a successful resident looks like to them.
- Letter of intent: After you’ve completed your interviews and before you submit your rank order list, send a letter of intent to your top few programs. They can double as thank you notes, which you should send to every place you interviewed.
Our Physician Advisors have helped thousands of med students stand out in their residency interviews. Learn how 1-on-1 interview prep from MedSchoolCoach can help you match into your dream program.
Ranking Your Programs
Creating a rank order list is straightforward but requires important decision-making. Only rank programs that you would actually accept an offer from. Rank your most ideal programs at the top.
Important to know — don’t try to game the system. Both the NRMP and AAMC have advised applicants to create a rank order list of their true preferences, not how they think they will match.
The final rank order list is due at the end of February to prepare for Match Week in March.
Read More In-Depth: Rank Order Lists (ROLs) + How to Boost Your Odds on Match Day
Couples Match on the ROL
The Couples Match is for any two individuals who want their match to be contingent on where their partner matches. Really, you don’t have to be romantically involved with the other person — you can Couples Match with anyone, although I wouldn’t recommend it.
The Match algorithm only matches couples as a pair, not individual programs. Here’s how the Couples Match process works, in a nutshell:
- You and another person must couple on the NRMP’s R3 system. There is a small fee.
- Your rank order lists (ROLs) will be linked – as in, your #1 rank will only result in a match if their #1 rank will result in a match, and so on.
- You may list the same residency multiple times. In fact, I recommend listing a desired program multiple times, each time pairing it with a different program on your partner’s ROL.
- You may list “No Match” if you’re willing to go unmatched and let your partner match. I suggest saving any “No Match” codes for near the bottom of your ROL. If a “No Match” is near the top of your list, your chances of not matching go up when the risk may not be necessary.
There is absolutely no requirement to have the same specialty or the same location. There are many reasons you might pair programs where you interviewed with programs where your partner interviewed. Just keep the “No Match” codes for the end of your ROL.
If you or your partner is applying to an advanced program (PGY-2), you’ll need to add a supplemental rank order list. Fees may quickly stack up when adding supplemental ROLs for preliminary or transitional programs.
Learn More: Categorical vs. Preliminary vs. Advanced Residency Programs
Contiguous Ranks on the ROL
Contiguous ranks are the number of specialties that appear in a row on your rank order list (ROL).
Below are a couple of examples of how to use contiguous ranks to your benefit. You can either prioritize one specialty over others (Example A) or prioritize the program over what specialty you go into (Example B). Choosing one method over another can help you during Match Week.
Example A: Applicant A may be particularly interested in dermatology, so they use a very contiguous list of preferred programs.
Applicant A:
Derm program 1 Derm program 2 Derm program 3 Pediatrics 1 Pediatrics 2
Example B: Other students may have multiple specialty interests and use a non-contiguous list instead. This method may indicate you care more about the program than the specialty, which is totally fine.
Applicant B:
Derm program 1 Pediatrics 1 Derm program 2 Pediatrics 2 Derm Program 3
Both applicants have 3 Derm programs and 2 Pediatrics programs. Applicant A has 3 contiguous ranks for Derm and 2 contiguous ranks for Pediatrics. Applicant B has no contiguous ranks.
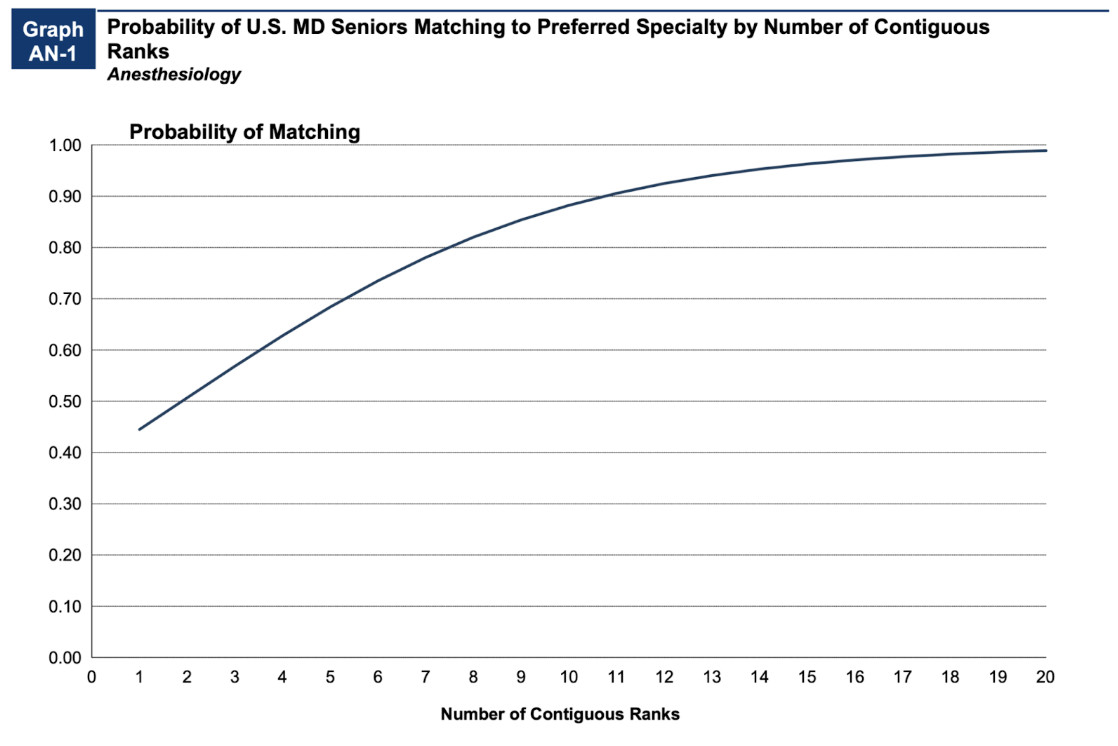
The number of contiguous ranks is important. For example, anesthesiology applicants with 12+ contiguous ranks matched with an anesthesiology program 90% of the time. But applicants with only one contiguous rank matched less than 40% of the time.
However, you can still rank multiple specialties. The data from previous years have mixed match outcomes, depending on the specialty. Research the match data about the specialties you’re considering to make a decision on your preferred specialty and how to rank your list accordingly.
Related: Medical Specialties with Good Work/Life Balance and Low Burnout Rates
Match Week
Residency Match Week occurs every March. (In 2026, it’ll be March 16-20.) It’s when several important residency-related events happen:
- On Monday of Match week, you figure out whether or not the NRMP algorithm matched you with a residency program. (But not where you matched.)
- If you didn’t match, you’re likely eligible for SOAP. Learn more in the next section.
- SOAP-eligible applicants can choose to apply to unfilled positions. There are four rounds of SOAP offers on Thursday of Match Week.
- On Friday of Match Week, you figure out where you matched.
SOAP: Supplemental Offer and Acceptance Program
The SOAP (Supplemental Offer and Acceptance Program) is designed to fill in the gaps left by the algorithm for applicants who didn’t get matched and for program spots that didn’t get filled.
On Monday of Match Week, applicants are notified if they are eligible for SOAP. To be eligible for SOAP, you must be:
- Unmatched
- Registered in the main match through NRMP
- Available to start residency in June
SOAP works in a completely different way from the NRMP. There is no algorithm for SOAP at this time, and the process happens very quickly.
SOAP-eligible applicants can access a list of all the unmatched program positions through the NRMP website. There, you can apply to as many as 45 programs via ERAS.
The programs may interview you by phone over the next couple of days. You’re not allowed to contact programs during this time unless they initiate contact with you. Programs, not applicants, submit a new rank order list of candidates they’ve interviewed.
Based on these lists, SOAP offers are extended on Thursday of Match week. There are four rounds of offers — each lasting two hours, during which you can accept or reject an offer, with one hour between each round for the algorithm to determine the next set of offers.
- Round 1 of SOAP begins at 9 AM ET.
- Round 2 at 12 PM ET.
- Round 3 at 3 PM ET.
- Round 4 at 6 PM ET.
Most SOAP positions are filled in round 1. Any applicants who go unmatched in Round 1 move on to Round 2 and so on, until the conclusion of Round 4 at 8 PM ET.
Once SOAP ends on Thursday evening, applicants who are still unmatched receive a final list of unfilled programs. Now, the rules change: You may contact the programs on that list and ask for interviews. They can extend an offer to you at any time before the end of the application cycle.
This post-SOAP process is typically available from Thursday of Match Week until May 1st — about 5-6 weeks.
Read more about SOAP on the NRMP’s website.
Important Notes for IMGs
International medical graduates (IMGs) are at an inherent disadvantage compared to American medical graduates for multiple reasons. What determines whether you are an IMG is whether you attended or graduated from a school of medicine outside the U.S., not where you were born.
Note: For medical school graduates in the class of 2026 and beyond, Canada and the USA will no longer practice reciprocity and will consider graduates of the other country as IMGs.
Most program directors are familiar with and confident about the medical education that US medical graduates receive. However, many programs view IMGs as somewhat of an unknown since international standards can vary significantly. Plus, there’s already a large pool of applicants for just a few positions.
IMGs need to show more competitiveness. That means higher USMLE scores, more research and clinical hours, and more volunteer activities — anything that gives your application an edge.
Important: There are IMG-friendly states and IMG-friendly programs. I suggest looking at the data to identify residencies that are more likely to accept IMGs. Avoid highly ranking programs that have a history of not accepting international graduates.
Once you’ve identified which states/programs match IMGs into the specialty of your choice, the next step is to look at the Residency Explorer tool to specifically find out how many IMGs match into specific programs.
Related: How IMGs Can Match Into Their Ideal Residency
FAQs
Although not every residency participates in program signaling, you may increase your odds of desired match results by using program signals to indicate your interest and stand out from the crowd of applicants.
Read more about residency program signals in this free guide or on AAMC’s website.
Several factors make you a more competitive applicant in the residency match, such as:
- High USMLE Step 2 CK score
- High med school GPA
- 300+ clinical hours
- 300+ research hours
- Impressive extracurriculars, including a lot of shadowing
Strong personal statement on your ERAS
The ERAS residency application cycle opens in early June, but you can’t start submitting applications until September.
Although you may submit applications through winter, you’re much more likely to get an interview invite and later get matched if you apply early. We recommend applying within 1-2 weeks of when ERAS allows you to actually send applications.
The NRMP Match algorithm works by trying to match applicants to preferred programs and programs with their preferred applicants. It aims to make as many people happy as possible.
Example: If your #1 ranked program has also ranked you, you are marked as a tentative match. You may be unmatched if another candidate lists that program on their ROL and the program has that applicant higher on their ROL.
Learn more about the Match algorithm on the NRMP website.
Navigate through the NRMP website to the R3 system (the LOG IN/REGISTER button). First-time users will receive an email with a unique token link.
On this R3 website, you can make your rank order list and view Match information.
Maximize Your Odds on Match Day
The residency application process is a long road that requires planning. What’s more, close to 20% of applicants don’t end up matching into a PGY-1 position.
Stay ahead of the curve by investing in 1-on-1 mentorship throughout the residency application process, from carefully selected audition rotations all the way to Match Day.
We match 99% of US clients and 88% of IMG clients into residency. Build your application alongside a Physician Advisor with admissions committee experience.

Amar Mandalia, MD
Dr. Mandalia is an accomplished medical writer with multiple manuscripts in peer-reviewed journals and a practicing GI physician in the Orlando area. He is the Admissions Advisor for MedSchoolCoach and has extensive experience helping students get into medical school and residency.
See How We Can Help
Search for:
RECENT POSTS
Medical Schools in Illinois
medschoolcoach
What Are the COMLEX-USA Exams?
Joel Ramirez MD
The Ultimate Guide to Medical School Scholarships
medschoolcoach
2025/26 Casper Test Dates & Schools That Require It